

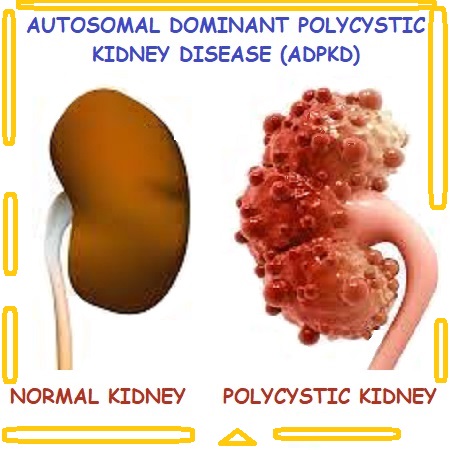
Autosomal dominant polycystic kidney disease (ADPKD) is among the most hereditary diseases. The disease has variable penetrance but accounts for ten percent of Dialysis patients in the United States.
Abdominal or flank pain and microscopic or gross hematuria are present in most patients. A history of urinary tract infections and nephrolithiasis is common. The combination of hypertension and an abdominal mass should suggest the disease. 40%-50% have concurrent hepatic cysts pancreatic and splenic cysts may occur. Hemoglobin tends to be maintained as a result of erythropoietin production by the cysts. The urinalysis may show hematuria and mild proteinuria.

TREATMENT
Hematuria is most commonly due to rupture of a cyst into the renal pelvis but it can also be caused by a kidney stone or UTI(urinary tract infection). hematuria typically resolves within seven days with bed rest and hydration.
Abdominal or flank pain is caused by infection, bleeding into cysts, and nephrolithiasis. Bed rest and analgesics are recommended. Cyst decompression can help with chronic pain.
An infected renal cyst should be suspected in patients who have flank pain , fever and leukocytosis. Blood cultures may be positive and urinalysis may be normal if the cyst does not communicate directly with the urinary tract . CT scan may be helpful because infectious cysts may increase wall thickness. Antibiotics use in cystic infection is fluoroquinolones or trimethoprim-sulfamethoxazole.
In nephrolithiasis up to 20% of patients may have kidney stones, mainly calcium oxalate , Hydration approximately 2 to 3 Liter per day is recommended in order to prevent precipitations of stones .
For Informational purpose only. Consult your Physician for advice.